Global Health Expenditure is Increasing…
A recent global health report from IHME[1] reported that global health expenditure had reached a whopping $8.4 trillion in 2018. The majority of this (59.4%) was government health spending. However, prepaid private spending accounted for almost a quarter (22.1%). Many people pay directly for some, or all, of their healthcare when they need it, and this accounted for a further 18% of global health spending. Less than one percent (0.5%) was accounted for by donor finance.
Projections suggest that global health spending is expected to increase to $14.4 trillion by 2050. After allowing for population growth that amounts to a 38% increase in global spending on health.
Drivers of growth in health spending
There are many drivers of growth in demand for health, and hence the need for health finance. The most important are:
- Growth in the size of the population.
- Changes in the demographic profile of the population with costs generally being highest at times of birth, pregnancy, and the last years of life.
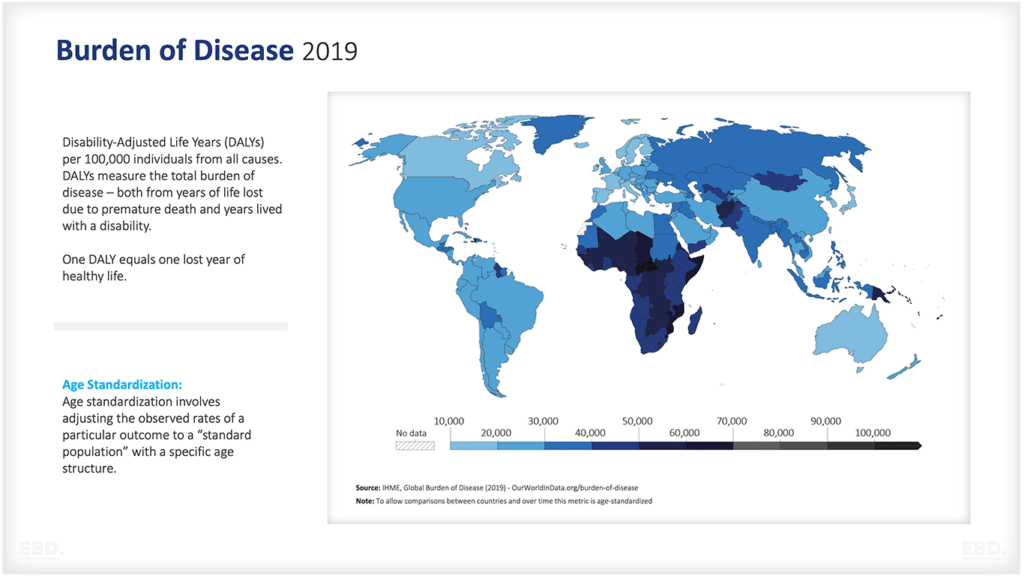
- The incidence and prevalence of diseases that are infectious or transmissible across the population – otherwise known as a communicable disease. Examples here include tuberculosis, HIV/AIDS, Hepatitis B etc.
- The incidence and prevalence of diseases that are not transmissible, but which impact heavily on population health, especially when combined with each other or natural frailty which comes with age – otherwise known as non-communicable disease. Examples here include heart disease, diabetes, osteoarthritis etc.
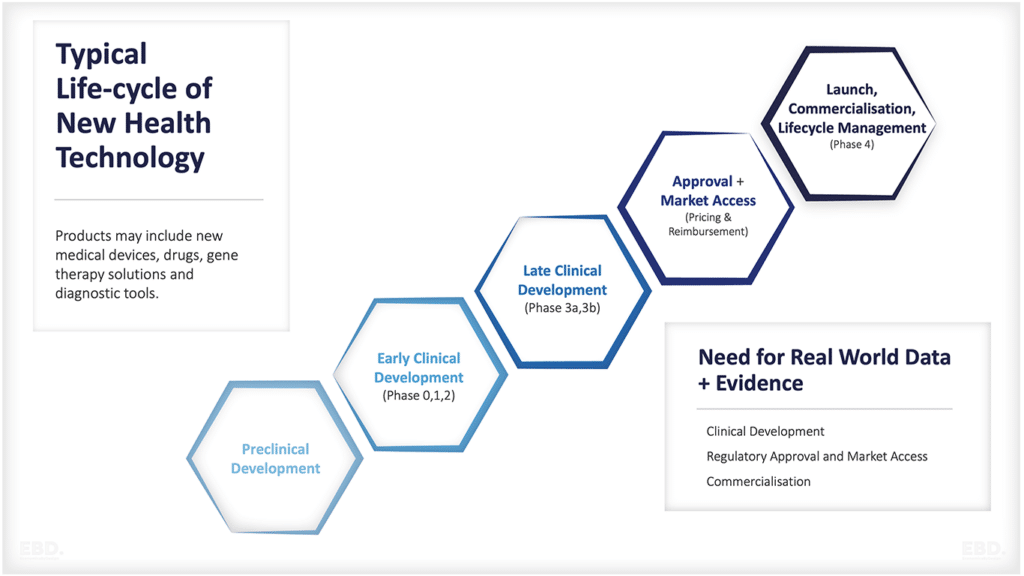
- The availability of new diagnostics and treatments and innovative drugs.
Given that over 80% of health spending is government or pre-paid private spending, growth in health demand will put pressure on health financing and hence the tax-payer and those individuals contributing to health insurance. Governments and insurance companies can respond in a number of ways:
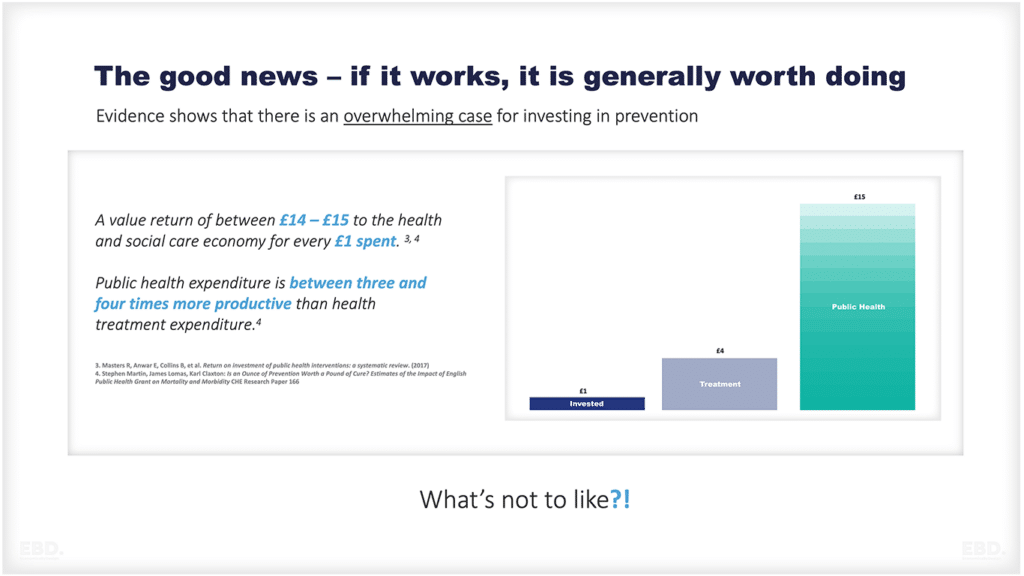
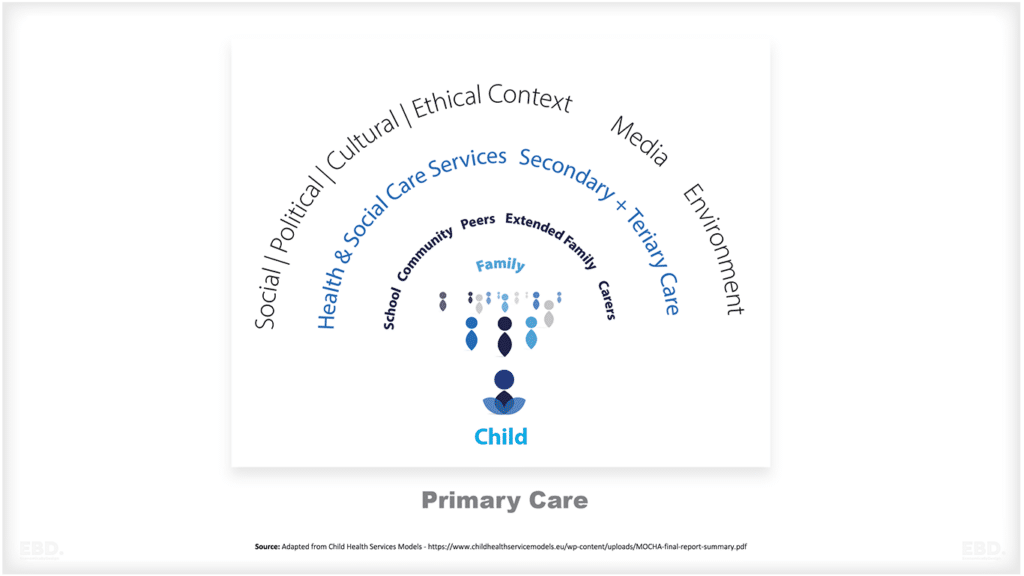
Investing in wellness and primary prevention
Investing in secondary prevention to help people to live well with chronic disease
Promoting the efficiency of health systems through
- on-going productivity initiatives
- strategic purchasing from groups of providers to benefit from economies of scale and scope
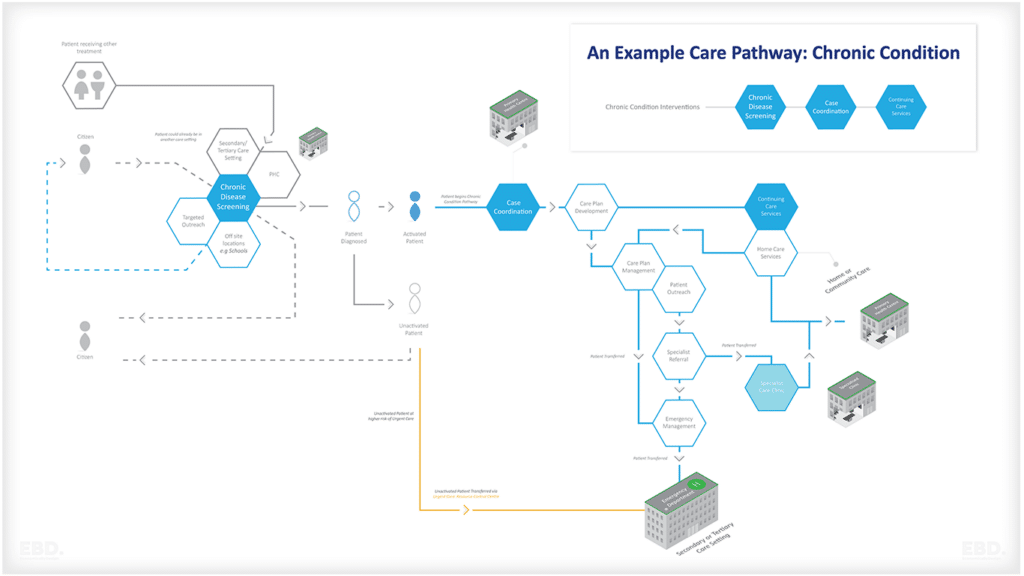
- integrated care to ensure efficient care coordination across complex pathways
- health technology appraisal to ensure value for money of new health diagnostics and treatments
Increasing the contribution from taxpayers and insured populations.
Ultimately, “enough” will be determined by societies and individuals’ perceived value of health and their willingness to pay for healthcare.
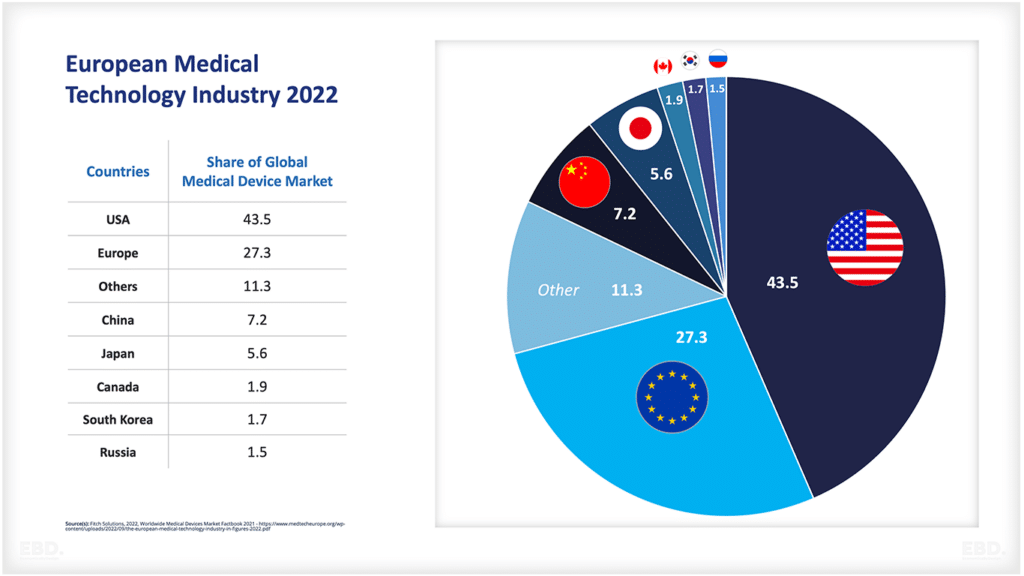
This will be influenced by the wealth of a country, which is why we often compare health spending across countries as a percentage of GDP. For high-income countries, we are edging close to ‘enough’, or at least ‘enough given our economic wealth’.
The big elephant in the room, however, remains global economic inequality and low-middle income countries where health financing is not supported by insurance or government protection.
Without the protection of universal coverage and associated financial protection from governments or insurance companies, individuals faced with life-threatening expensive diseases like cancer either go without, or experience catastrophic health expenditure.
Sadly, there remain huge gaps in terms of health coverage and health financing, with populations in many low to middle-income countries having to pay for healthcare directly when it is needed (out-of-pocket). While the global figures suggest around 18% of health spending is out-of-pocket, there are many countries with much higher figures.
World Bank data suggest the following countries all have out-of-pocket health spending in excess of 70% of overall health expenditure [3]:
- Armenia
- Afghanistan
- Turkmenistan
- Myanmar
- Equatorial Guinea
- Bangladesh
- Cameroon
- Tajikistan
- Nigeria
Shifting from out-of-pocket payments to health insurance or tax funded services would spread the risk much more effectively and improve life expectancy.
The Institute for Health Metrics and Evaluation (IHME) report suggests that, without action, these global health financing disparities are unlikely to have changed much by 2050. Universal health coverage, enabled by health financing reform, should therefore remain a priority of international agencies such as the World Health Organisation and the World Bank, if we are to reduce global health inequalities.
[1] //www.healthdata.org/sites/default/files/files/policy_report/FGH/2021/FGH_2020_full-report.pdf
[2] Graph Source IHME; ID856380